

Leadership
Faculty celebrated for leadership, advancing medicine, research and training to serve others
The National Drug Abuse Treatment Clinical Trials Network (CTN) is a means by which medical and specialty treatment providers, treatment researchers, participating patients, and the National Institute on Drug Abuse cooperatively develop, validate, refine, and deliver new treatment options to patients. This unique partnership enables the following:
Celebrating 25 Years of Research-Practice Partnerships
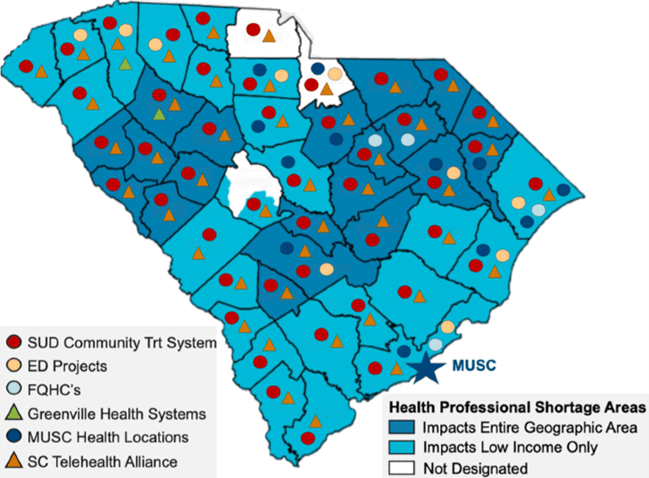
The SCN team has developed deep and robust statewide collaborations. We work closely with the South Carolina Department of Alcohol and Other Drug Abuse Services (DAODAS), community treatment programs state-wide, the state legislature, the SC Department of Health and Human Services (DHHS) and medical providers throughout the state (FQHCs). We also have strong affiliations with healthcare systems and other research Universities statewide as well as the South Carolina AHEC system.
The SCN's regional partners in Georgia, Alabama, Mississippi, Louisiana and Northern Florida are located in primarily rural areas with overall health rankings in the lowest quartile in 2018. The poverty rate in these states is higher than the national average, and all have, on average, over 10% uninsured population. Over 60% of designated Primary Care, Dental Health and Mental Health Professional Shortage Areas (HPSAs) in the United States are in rural areas. For all six states in our consortium, the vast majority of counties are considered HPSAs for both primary care and mental health. Additionally, 5 of the 6 states in our consortium are non-Medicaid expansion states.
The opioid epidemic has drawn particular attention to the shortfall of mental health and SUD treatment providers and facilities in rural areas. Both historically and currently, the southern US has the greatest substance use services disparities and facilities that provide comprehensive SUD treatment services are extremely limited. Unique barriers to recovery for individuals in rural areas include geographic proximity to services, transportation difficulties, financial burden and stigma/privacy concerns in small towns. Technology, particularly home-based tele-visits, can play a critical role in overcoming some of these barriers.
Although the findings from SCN studies will have broad applicability to the treatment of SUD in a variety of settings nationwide, we will make addressing the pressure points across the continuum of care for SUDs a primary focus of the SCN research agenda.
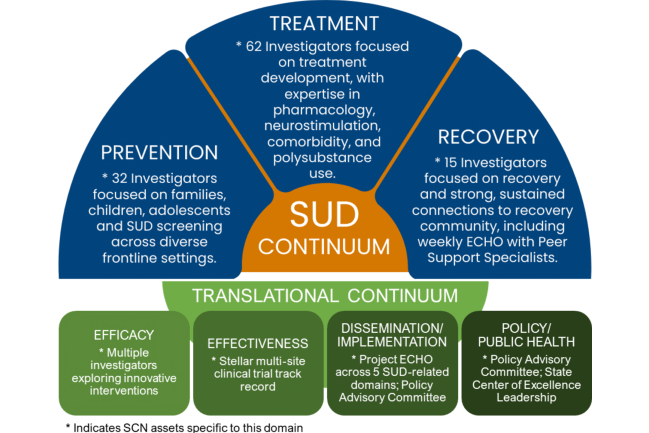
The SCN research agenda focuses on developing and testing emerging evidence-based interventions that address substance use issues spanning the SUD continuum: prevention, treatment, recovery.
Over the past 24 years, the Southern Consortium Node (SCN) has been an integral part of the NIDA Clinical Trials Network (CTN), participating comprehensively in CTN activities and expanding our impact, geographic reach and research practice settings. Over the next seven years, we propose to address research questions focused on critical gaps along the substance use disorder (SUD) treatment continuum, from prevention to recovery, culminating in implementation science to ensure real world impact. Our highly experienced team will leverage the successful SCN research infrastructure and local, regional, and national collaborators to propose, participate in and lead groundbreaking multi-site trials to improve prevention, treatment, morbidity and mortality for those affected by SUDs.
The primary aims of the SCN are:
Below are additional resources for addiction treatment, training and research.
The MUSC CTN team consists of clinical and scientific experts from diverse and complimentary specialties. The common mission among our faculty and staff are to contribute to the advancement of treatment for addictions through the conduct of innovative and rigorous clinical trial research.

Dr. Kelly Barth is a Med-Psych physician board-certified in internal medicine, addiction psychiatry and pain medicine. She directs the MUSC Pain Rehabilitation Program and also performs research in the area of opioid tapering and peer-led interventions for opioid overdose survivors. She is a member of the MUSC Project Echo OUD Hub where she provides mentoring and lectures in the areas of addiction diagnosis and treatment, pain management, and overdose prevention.

Kathleen T. Brady, M.D., Ph.D., is a clinical and translational researcher with more than 30 years of experience at multiple levels in the translational research spectrum. Her research focuses on the development of new treatments for individuals with substance use disorders, with an emphasis on translating study findings into effective treatment interventions. She began her research career conducting basic science work in the drug abuse field and received her Doctor of Philosophy (Ph.D.) in Pharmacology.
Dr. Brady moved into clinical and translational research after finishing her residency in psychiatry in 1989. She has been continuously federally funded to conduct research since 1989. Her recent research activities involve the interface between basic and clinical science investigating the mechanistic connection between stress and substance use disorders and in the translation of empirically-based treatments from academic medical centers to front-line treatment settings.

Professor of Psychiatry and Behavioral Sciences

Louise Haynes is an assistant professor in the Department of Psychiatry and Behavioral Sciences at the Medical University of South Carolina. For the last sixteen years, she has served as a liaison between academic research and community treatment programs for the Clinical Trials Network of the National Institute on Drug Abuse. In addition to her research experience, Ms. Haynes has worked in both clinical and administrative roles in South Carolina. She was Director of Women’s Services for the South Carolina Department of Alcohol and Other Drug Abuse Services and, later, the Director of Morris Village, a residential treatment program in Columbia.

Professor of Psychiatry and Behavioral Sciences

Dr. McCauley is a clinical psychologist who has led efforts to disseminate best practices in opioid prescribing to dental professionals. She will head up the Health Care Systems Liaison Core.
Dr. McCauley's general research interests focus on the dissemination and implementation of multi-level interventions targeting prescription opioid abuse and its common comorbidities (e.g., pain, traumatic stress, depression). In addition, Dr. McCauley is an active collaborator on projects to develop, evaluate, and implement indicated prevention and early intervention programming for youth and adults at-risk for posttraumatic stress disorder (PTSD), substance use disorders, and HIV/STI.

Dr. Moreland is a clinical psychologist with expertise in adaptation, implementation and dissemination of evidence-based treatments. She is the co-lead investigator for CTN0107-A-1; she will lead the Community Liaison Core with Louise Haynes.

Constance Guille is the Director of the Women’s Reproductive Behavioral Health Division and Professor in the Department of Psychiatry and Behavioral Sciences at MUSC. Dr. Guille completed her psychiatry residency training and subspecialty training in perinatal psychiatry at Yale University. She established the Women’s Reproductive Behavioral Health Division at MUSC. She enjoys spending time with her husband and two daughters.
Dr. Guille has transitioned her research into the area of Perinatal Psychiatry investigating biological markers of postpartum depression. Her clinical practice focuses on the management of mental health problems in pregnancy and postpartum.

Dr. Erin A. McClure is a behavioral psychologist and an Associate Professor in the Department of Psychiatry and Behavioral Sciences at the Medical University of South Carolina. Dr. McClure earned her B.S. in Psychology and Neuroscience from Allegheny College and her Ph.D. in Psychology from the University of Florida. The overarching goal of Dr. McClure’s program of research is broadly focused on reducing the harmful impact of cannabis and tobacco/nicotine product use across the lifespan. Her research has focused on refining and evaluating strategies to improve long-term abstinence and prevent relapse, as well as pursuing harm reduction strategies to minimize the adverse impact of substance use; all utilizing technology to improve remote procedures and data quality, as well as to increase reach and accessibility.

Co-Investigator
wardrc@musc.edu
Dr. Ward is a statistician who will aid SCN investigators in conducting secondary data analyses of CTN studies. He will also provide statistical support in the development of SCN generated CTN concepts and protocols. He will work with Dr. Sonne on the Protocol Management and Administration Core.

Co-Investigator
jennil@musc.edu
Dr. Jennings is a physician in the MUSC Emergency Department. She is the site Principal Investigator for CTN0099 and the Co-Lead Investigator for CTN0107-A-1.

Dr. Karen Hartwell has extensive clinical experience as a general and addiction psychiatrist in the treatment of substance use disorders with/without comorbid psychiatric disorders. She was the Medical Director of the Substance Treatment and Recovery Program at the Ralph H Johnson VAMC until 2019. She has treated veterans with multiple substance use disorders, including opioids, alcohol, and stimulants, among others. She is now leading several initiatives to address the opioid epidemic, including becoming the medical director of MUSC’s Project ECHO Opioid Use Disorder program.
Dr. Hartwell made a mid-life career change and returned to academics to complete a fellowship in addiction psychiatry to better address the substance use disorders that commonly co-occur with psychiatric disorders. Her research career has focused on understanding the underlying neurobiology and improving treatment outcomes. She has collaborated on a variety of research studies involving opioids, cocaine, cannabis, alcohol, and tobacco use disorders. She has also been involved in multiple clinical trials, including multisite trials ranging from Phase 2 to Phase 4, investigating a variety of pharmacotherapeutic agents, and TMS.

Dr. Brown is a Research Assistant Professor in Addiction Sciences at MUSC. Her research focuses disparities in substance use disorders and comorbid stress-related conditions ( e.g., PTSD, trauma, early childhood adversity) that impact women and African Americans. She is currently examining the impact of race-related stress among individuals with alcohol use disorder and PTSD. She is also conducting a laboratory study to investigate sex differences in the impact of early childhood stress on opioid craving among men and women with opioid use disorder.

Dr. López’s research interests include identification of barriers to treatment engagement in mental health services, the use of culturally tailored interventions as a means of engaging specific high-risk groups in prevention and behavioral health services (e.g., HIV prevention, prevention of child maltreatment), increasing visibility and access of trauma related services to Latinx and other underserved populations (e.g. Telemedicine), and assessment of provider-level factors that affect youth and family involvement in outpatient community-based therapy.


The Innovation Sciences Unit is led by Dr. Jennifer Dahne, a Professor within the Addiction Sciences Division of the Department of Psychiatry & Behavioral Sciences. Dr. Dahne is an academic entrepreneur who has received five small business grants from various NIH institutes (NIMH, NIDA, NCATS, NIMHD) totaling more than $3M. Dr. Dahne has co-founded two faculty-led spinout companies, both of which are in the digital health space. Dr. Dahne has led the development, evaluation, and commercialization of five commercially available digital health products to date. These products have been evaluated via rigorous randomized clinical trials which have accrued more than 1,000 patients. In addition to entrepreneurial ventures, Dr. Dahne directs a research laboratory within the Addiction Sciences Division that has received numerous traditional NIH grant awards including R01, R21, and K23 funding. Dr. Dahne is passionate about translating academic innovations into products that can be widely disseminated and commercialized in order to improve public health.

Protocol Manager/QA Specialist
Ms. Shaw has been part of the SCN for over 6 years and has been involved in clinical research for approximately 9 years. Ms. Shaw currently acts as Protocol Manager/QA Specialist for CTN0100 and CTN0107, and acts as Program Coordinator for CTN0099.
The purpose the CTN Advisory Board is to enhance communication with key stakeholders in South Carolina and the broader region regarding emerging trends and challenges in the field, new areas for research, and guidance on the most effective ways to disseminate research findings to the community. The committee brings together a wide range of stakeholders, including payors, public administrators, health care providers from primary care and the specialty treatment system, and leaders from the recovery community.
Christina Andrews, Ph.D.
Associate Professor, Arnold School of Public Health
University of South Carolina
Jodi Manz, MSW
Executive Director at South Carolina Center of Excellence in Addiction
Allyson Sipes, Psy.D.
Inpt. Services Director of Clinical Services SC Dept. of Mental Health (SCDMH)
Michael Dennis, LPC
Executive Director
Tri-County Commission on Alcohol & Drug Abuse
Sara Goldsby, MPH, MSW
Director
SC Dept. of Alcohol & Other Drug Abuse Services
Melanie Hendricks, LISW-CP, ACSW
Director of Behavioral Health
South Carolina Dept. of Health & Human Services
Farrah Hughes, Ph.D., ABPP
Director of Behavioral Health Services
HopeHealth
Tricia Lawdahl, NBC-HWC
Director of Health and Wellness Initiatives
FAVOR Greenville
Taanya Mannain, LISW-CP
Director of Integrated Healthcare Services
Little River Medical Center
Kenyon Payton, MDiv, DMin
Pastor
New Bethel Missionary Baptist Church
Dawn Tyus, Ph.D.
Director
Southeast Addiction Technology Transfer Center
Susan Sonne, Pharm.D.
Investigator/Node Coordinator
sonnesc@musc.edu

